The Dark Legacy of Lobotomies
00:00:00
Speaker
Husbands would send their wives off to institutions and reported positive results after a lobotomy says she's restored.
00:00:06
Speaker
Leaves the house cleaner than ever before.
00:00:09
Speaker
Thank you so much, doctor.
00:00:10
Speaker
She's a better maid, sir.
00:00:14
Speaker
She just does what she's told.
00:00:15
Speaker
Her personality, gone.
Introducing 'Unpacking the Eerie' Podcast
00:00:22
Speaker
And I'm Shaina, and you're listening to Unpacking the Eerie.
00:00:26
Speaker
A podcast that explores the intersections of our dark and morbid curiosities through a social justice lens.
History and Realities of Asylums
00:00:42
Speaker
welcome to part two of our episode on Weston State Hospital.
00:00:47
Speaker
Thanks for coming back.
00:00:49
Speaker
If you are encountering this, not having listened to part one, please go back and listen to the episode right before this.
00:00:57
Speaker
There's tons of context that will be missing if you just jump in here.
The Evolution of Mental Health Institutions
00:01:02
Speaker
to refresh your brains, in the last episode we talked about how in the late 1800s, America would become home to a new wave of quote-unquote mental health institutions we now know as asylums.
00:01:15
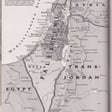
Speaker
The Weston State Hospital, aka the Trans-Allegheny Lunatic Asylum, which is the more disturbing name that the hospital is better known as, was one of many of these quote-unquote state-of-the-art facilities.
00:01:29
Speaker
In that episode, we talked about how aspirations for these palatial elite experiences for namely white mentally ill patients quickly descended into the picture that you probably have of these places, which are really just carceral sites of unspeakable cruelty and dehumanization for those who were multiply marginalized, who were forced to be there sometimes for their entire lives.
00:01:52
Speaker
There was so much information on this, we decided to break it up onto two parts.
00:01:56
Speaker
So in part one, we learned about why West End State Hospital is considered one of the most haunted places in the country, the history of asylums as a whole, and the social political climate that led to the extreme rise of people incarcerated in these institutions.
Sensitive Themes: Lobotomies, Misogyny, Racism, and Eugenics
00:02:12
Speaker
So this part two picks up right where we left off.
00:02:15
Speaker
Very briefly, as always, we want to state our content warning before jumping right into all of the material, just like the last episode.
00:02:24
Speaker
Part two has very similar themes.
00:02:26
Speaker
We'll be talking in depth about what was happening at these institutions, which includes details about
00:02:33
Speaker
lobotomies and other dehumanizing practices that were used at these asylums.
00:02:39
Speaker
We'll be talking about the rampant misogyny and racism that was occurring within these institutions, including conversations around eugenics.
00:02:50
Speaker
So as always, take breaks as you need, take care of yourself, consider yourself informed before jumping in, and thanks for listening as per usual.
Inhumane Treatments in Asylums
00:03:00
Speaker
makes sense that the only way to relate to those people is to control them.
00:03:05
Speaker
Anyway, that was, that was my, that was my addendum.
00:03:09
Speaker
That was kind of what was going on here.
00:03:11
Speaker
That was probably contributing to the rise.
00:03:14
Speaker
In the population.
00:03:15
Speaker
So yeah, thanks for giving us that context.
00:03:18
Speaker
Now I'm going to kind of go on to talk about the treatments that were being provided here, or quote treatments.
00:03:25
Speaker
Like I said before, cold baths, different kinds of hydrotherapy, electroshock therapy, insulin shock therapy, bloodletting, confinement cribs.
00:03:35
Speaker
and more, but I'm just going to give a little depth on what some of these were.
00:03:40
Speaker
So hydrotherapy was also known as the water cure, but it was essentially waterboarding because it was holding patients underwater in ice cold water until they lost consciousness after which they were considered cured.
00:03:55
Speaker
If they were, could be revived.
00:03:57
Speaker
Other forms were dunking or showering without warning.
00:04:01
Speaker
And it was often used on women who had a quote unquote diagnosis of hysteria.
00:04:06
Speaker
Insulin therapy, also known as insulin coma therapy, which is a form of psychiatric treatment in which patients were giving increasingly large doses of insulin to induce hypoglycemia or low blood sugar and put them in a coma.
00:04:21
Speaker
Based on the notion that the coma would jolt or shock them out of whatever psychosis they were in.
00:04:27
Speaker
It was discredited in the 1960s and stopped being used.
00:04:30
Speaker
But electroshock therapy started being used because it was actually cheaper than insulin therapy.
00:04:36
Speaker
And it's now known as ECT or electroconvulsive therapy.
00:04:40
Speaker
And at the time, electrodes were placed at the temples and electricity was passed through the temporal lobes to cause convulsions.
00:04:49
Speaker
And it often caused patients to wake up dazed or with amnesia, with headaches, with nausea, impaired intellectual function, memory, caused fatigue, and worked to subdue and make patients passive, essentially.
Electroshock Therapy: From Cruelty to Cure
00:05:03
Speaker
helped with psychotic symptoms, but only temporarily.
00:05:06
Speaker
So patients were often treated with electroshock therapy repeatedly.
00:05:11
Speaker
And it was very painful because they were given this therapy without any, like,
00:05:18
Speaker
Some patients were treated with it daily and a lot of these people eventually suffered serious brain damage with no hope of recovery.
00:05:29
Speaker
Because the treatments were so painful, before they began using paralyzing drugs,
00:05:36
Speaker
40% of patients suffered bone fractures from the wild thrashing that they had during the convulsions.
00:05:42
Speaker
After experiencing electroshock therapy like a few times, many patients made attempts to escape because they didn't want to face further treatments, which is super fair.
00:05:53
Speaker
A lot of people would tremble, sweat, and beg for help during these treatments.
00:05:59
Speaker
And they reported to their doctors that it felt like having a bomb fall on you or being in a fire and getting all burned up.
00:06:10
Speaker
So basically doctors believed that electroshock made psychotic symptoms disappear and depression disappear, even if it hindered the patient's ability to think and remember for a time.
00:06:22
Speaker
And they felt that they had a right to administer it to even unwilling patients.
00:06:26
Speaker
And it remained a common procedure for two decades.
00:06:30
Speaker
Hospitals found that it helped to quiet patients.
00:06:33
Speaker
the wards and was a sedative for people that were disruptive.
00:06:37
Speaker
Interestingly, it's actually still a procedure that people can go through, but it's done under general anesthesia now and the electric currents are much smaller.
00:06:48
Speaker
So it's much safer of a treatment today.
00:06:51
Speaker
And it's used to treat severe depression, mania, catatonia, agitation and aggression in people with dementia.
00:06:58
Speaker
I mean, it makes sense that you would want to stimulate electrical signals in the brain because our brain is electricity.
00:07:05
Speaker
But yeah, the history behind how what's now known as electroconvulsive therapy is big yikes, very scary.
00:07:16
Speaker
And then what are some of the other ones that I said?
00:07:20
Speaker
Bloodletting, which is essentially just withdrawing blood from a person's veins.
00:07:25
Speaker
And they believed it would rid the body of impure fluids.
00:07:29
Speaker
And then confinement cribs.
00:07:33
Speaker
Confinement cribs were just used to restrain adult patients.
00:07:36
Speaker
And they're essentially, they're also known as Utica cribs.
00:07:40
Speaker
And they were long and narrow up to 15 to 30 inches high.
00:07:43
Speaker
A person couldn't either sit up or get up in it.
00:07:46
Speaker
They had to lie down.
00:07:48
Speaker
I looked at pictures of it and it essentially looks like the skeleton of a coffin.
00:07:52
Speaker
Like it looks like it's shaped like a coffin, but.
00:07:54
Speaker
you can see out of it.
00:07:55
Speaker
It's like a cage, essentially.
00:07:57
Speaker
That was also another way that they used to subdue their patients.
00:08:02
Speaker
So it was up till basically the mid-1950s that
Kirkbride Asylums: Oversight and Overcrowding Issues
00:08:06
Speaker
these treatments were being used a lot.
00:08:09
Speaker
So similar to Weston State Hospital, Kirkbride Asylums were left completely unaccountable, right?
00:08:15
Speaker
They evolved invisible to the public eye with no oversight.
00:08:19
Speaker
Very similar to the setup here, they often held triple the number of intended patients with only one doctor to tend to residence, and
00:08:27
Speaker
and the doctors were ill-equipped, and they didn't know much about the brain at all in the early 1900s.
00:08:33
Speaker
The brain is a mystery today.
00:08:34
Speaker
The brain was an extra mystery.
00:08:38
Speaker
And the states responded to the overflow by constructing more giant facilities.
00:08:42
Speaker
Pilgrim State, for example, held 13,000 people.
00:08:47
Speaker
Experimental treatments, just like the ones at Weston State Hospital, were done everywhere.
00:08:51
Speaker
Wet pack, chemically induced seizures, hot box, chemically induced comas, wet shock, hydrotherapy, fever therapy.
00:08:58
Speaker
That's just a few.
00:09:01
Speaker
In 1927, an Austrian doctor won a Nobel Prize for malaria therapy.
00:09:09
Speaker
When patients developed a fever, they appeared better, is what they noticed.
00:09:14
Speaker
And so they would take blood from malaria victims and then inject it into patients who had psychosis.
00:09:20
Speaker
Oddly enough, it did help alleviate symptoms for some psychoses, the ones caused by syphilis in particular.
00:09:26
Speaker
It was because the high fever was killing the microorganism in the brain that was causing it.
00:09:31
Speaker
Treatment failed for other people, for other ailments, and then sometimes they killed people.
00:09:35
Speaker
So it was just trial and error at the expense of people's lives.
00:09:40
Speaker
Because these facilities promised to families that they'd be able to cure people upon admission, which is why families were so eager to give up their loved ones.
00:09:48
Speaker
I mean, sometimes it was about control, but sometimes it genuinely was like, I don't know what to do about this family member who seems to be really needing help.
00:09:55
Speaker
And then they'd be stuck in a situation where they're being tortured, sometimes to death.
00:09:59
Speaker
But because Kirkbride, his whole thing was, you take people in, you cure them, they go back out.
00:10:05
Speaker
One of the reasons why there were so many overflowing...
00:10:09
Speaker
facilities was because that was untrue.
00:10:11
Speaker
People never left.
00:10:13
Speaker
They were like dying or getting worse.
00:10:17
Speaker
Because they were being harmed.
00:10:20
Speaker
And so because they couldn't fulfill that promise, they told families that the ones who could not be cured were defective degenerates and they were not fully human.
00:10:29
Speaker
Not like, it's our fault.
00:10:31
Speaker
Because we don't know how to treat this person.
00:10:33
Speaker
Yes, because... And that we're harming them, torturing them, abusing them.
00:10:37
Speaker
Yeah, because these families had money.
00:10:39
Speaker
Right, like they had power to do something about that.
00:10:43
Speaker
A lot of the time, not always, the publicly funded ones were different, but these practices were being used across the board.
00:10:49
Speaker
This was like the beginning of a different set of discourse around...
00:10:55
Speaker
people who were mentally ill.
00:10:56
Speaker
Not that the discourse has been positive.
00:10:59
Speaker
But this idea that Kirkbride was like, oh, these are like places for, you know, rejuvenation and care and people deserve to be living in these lush environments.
00:11:09
Speaker
You know what I mean?
00:11:10
Speaker
Like that, that was like completely taken away at this point.
00:11:13
Speaker
And staff would abuse people.
00:11:17
Speaker
And that, yeah, most of those staff were like overworked, underpaid, undertrained.
00:11:24
Speaker
for these positions and they were living there too so yeah so like the evolution of this language becomes increasingly callous and cruel and dehumanizing and i think that this is really paralleled with the eugenics narratives in that article that i was quoting earlier they were saying that psychiatric discourse about black patients in particular
00:11:45
Speaker
at the end of the 19th century centered around false ideas of biological difference and inherent deviance, setting the scene for a century of neglect, underfunding, and abuse."
00:11:53
Speaker
And so this language is also what caused people to withdraw funding and prioritization for
Forced Sterilization and Eugenics in Asylums
00:12:02
Speaker
these institutions.
00:12:03
Speaker
In paperwork during this time, you also see that they're not called patients anymore, they're called inmates.
00:12:10
Speaker
And then this is also when they started forced sterilization on anyone who was confined to the institution.
00:12:15
Speaker
Laws across the nation began to adopt this into practice, basically saying that if an institution deemed it was necessary or appropriate to be sterilizing people,
00:12:27
Speaker
patients that they could do it without their consent and without their knowledge.
00:12:31
Speaker
So people would be going in for different treatments, thinking that they were going to be treated for something else, and they could come out sterilized without their knowledge at all.
00:12:42
Speaker
And forced sterilization was very much fueled into practice by eugenics.
00:12:47
Speaker
Eugenics was a framework that was started by Francis Galton, who was related to Charles Darwin.
00:12:55
Speaker
He believed that, quote-unquote, genetically feeble people should eventually be winnowed from the future, which was on the basis of race, gender, and ability, the intersection of all of those things.
00:13:06
Speaker
And this is where social Darwinism comes in and stuff.
00:13:09
Speaker
Thousands of patients during this time were sterilized on the whims of eugenics-based assessments, and
00:13:16
Speaker
In this PBS documentary that I was watching, they had scans of asks for donations, which was kind of eerie because it really mirrors the way we ask for donations for modern day nonprofits.
00:13:31
Speaker
Not using the same language, but it had the same vibe, you know?
00:13:33
Speaker
And it's really offensive.
00:13:35
Speaker
But it says, some people are born to be a burden on the rest.
00:13:40
Speaker
That's the heading.
00:13:43
Speaker
Every 15 seconds, $100 of your money goes for the care of persons with bad heredity, such as the insane, feeble-minded, criminal, and other defectives.
00:13:55
Speaker
Here we have this shift of, oh, we're taking care of all of these people and we're fixing them and we're going to make them better for society, which is a problem in and of itself.
00:14:04
Speaker
And there's this shift in language to be like, your money is going to get rid of people who shouldn't be here anymore, is the language.
00:14:14
Speaker
Circling back to the article written on racism in asylums, she says, it's not simply that Black patients were routinely provided with less rations, less clothing, and inferior buildings, but
00:14:24
Speaker
but that these conditions were supported by ideologies of eugenics and mental hygiene, justifying the long-term confinement and reproductive sterilization of thousands of people whom the elected politicians of Georgia – they were doing a case study on an asylum in Georgia – whom the elected politicians of Georgia saw as little more than burdens on the state.
00:14:44
Speaker
And then it talks about how the Binet IQ test was launched during this time.
00:14:48
Speaker
And we still use IQ test as a measure of intelligence, right?
00:14:53
Speaker
It was devised and used to justify eugenics narratives.
00:14:56
Speaker
And then they use that to push forward sterilizations, saying, look, look at these people, incapable, shouldn't be reproducing.
00:15:04
Speaker
I mean, those tests are also not built for neurodivergent folks in any way.
00:15:11
Speaker
I remember I took one of those tests when I was in middle school or high school and I got a pretty low score and I was like, why am I getting such a low score on the IQ test?
00:15:22
Speaker
Yeah, it's just arbitrary.
00:15:24
Speaker
And I mean, I wonder whether a lot of standardized tests...
00:15:28
Speaker
They're rooted in the history of this IQ test as well, because a lot of them hold similar problems.
00:15:35
Speaker
And then are a way to, you know, marginalize folks further if they're not able to perform a certain way on them.
00:15:41
Speaker
I mean, that's its origin story.
00:15:43
Speaker
To be able to use, in the name of science, a way to categorize people in a definitive way as less worthy, less human, and disposable.
00:15:55
Speaker
So, you know, that.
00:15:58
Speaker
Which brings us forward to lobotomies.
00:16:02
Speaker
What are lobotomies?
00:16:06
Speaker
Well, in 1936, this dude in Washington, DC, Walter Friedman, performed the first lobotomy
00:16:14
Speaker
People thought this shit was a miracle.
00:16:18
Speaker
People in psychosis lost their paranoias, their hallucinations, and delusions while being able to function more or less.
00:16:25
Speaker
And many people were discharged after, so doctors thought the tradeoff was pretty worthwhile.
00:16:31
Speaker
Because they're like, these places are overrun, we're not curing people, we're stuck, people are not funding us anymore, yada yada yada.
00:16:38
Speaker
So this was like a way that all of a sudden psychiatry was rebuilding a name for itself, I guess, among the elite.
00:16:45
Speaker
I forget this dude's name, but there was an incident.
00:16:49
Speaker
Do you remember the psych study we talk about?
00:16:52
Speaker
Him in, like, Psych 101.
00:16:54
Speaker
But basically, he's, like, working, and then he gets a rod through his head.
00:16:58
Speaker
And then they were like, he should be dead, but he's not.
00:17:01
Speaker
There's a rod through his head.
00:17:02
Speaker
But it just, like, messed his personality up.
00:17:04
Speaker
It just fucked up his personality, yeah.
00:17:06
Speaker
But, you know, this was the first time that they had considered, oh, maybe the personality part of our brain sits in our... Phineas Gage.
00:17:13
Speaker
Phineas Gage, yes.
00:17:16
Speaker
I saw his skull when I worked at a neuroscience lab.
00:17:20
Speaker
We like went there on a lunch break because it was on the same, it was on the Harvard Medical School campus.
00:17:27
Speaker
Yeah, they have a skull.
00:17:28
Speaker
The Harvard Medical School Museum.
00:17:31
Speaker
Wow, you were there.
00:17:32
Speaker
You were in the origin story place.
00:17:35
Speaker
Well, basically, yeah, they were like, oh, look at this.
00:17:38
Speaker
People are still alive, wandering about.
00:17:40
Speaker
They're a little weird now.
00:17:42
Speaker
But they can still live.
00:17:43
Speaker
So they were like, wow, maybe our personality is stored in the frontal lobe, which, you know...
00:17:50
Speaker
Our frontal lobe controls executive functioning, critical thinking.
00:17:55
Speaker
Conscious brain, yeah.
00:17:56
Speaker
Allows us to process complex thoughts, whatever.
00:18:00
Speaker
But anyways, people are like, wow, lobotomy is amazing.
00:18:05
Speaker
Columbia, Harvard, Yale start these programs.
00:18:09
Speaker
called psychosurgery programs, which are basically just lobotomy programs after this.
00:18:15
Speaker
As to be expected, far more women were lobotomized than men.
00:18:18
Speaker
Husbands would send their wives off to institutions and reported positive results after a lobotomy.
00:18:23
Speaker
Says, she's restored.
00:18:25
Speaker
Leaves the house cleaner than ever before.
00:18:27
Speaker
Thank you so much, doctor.
00:18:33
Speaker
She's a better maid servant.
00:18:35
Speaker
She does not speak back to me anymore.
00:18:38
Speaker
Just does what she's told.
00:18:38
Speaker
Her personality, gone.
00:18:41
Speaker
That's exactly, that's all I ever wanted.
00:18:44
Speaker
All I wanted was a vessel.
00:18:46
Speaker
And here I have one.
00:18:51
Speaker
anyway honestly men still want that yeah and i found out that like you know the now there's ai girlfriends or whatever and there's data that shows the very first thing that most men do is emotionally abuse them what's wrong with them i don't know what's wrong there's something so wrong with them and sex robots what's that yeah what is that sex robots are like a
00:19:17
Speaker
extension of the blow-up dolls yes it is an extension of the blow-up dolls which is a whole nother ethical discussion in and of itself yeah and i wouldn't have such a problem with it if men didn't already see women as blow-up sex dolls as objects as objects yeah literally there's these studies that show did we talk about this study i think that you already mentioned it yeah study about brain scans yeah and how literally yeah that they just look
00:19:43
Speaker
The same as when they're looking at objects.
00:19:45
Speaker
When they look at women.
The Procedure and Impact of Lobotomies
00:19:50
Speaker
increased in popularity.
00:19:52
Speaker
People were all about it.
00:19:53
Speaker
But neurosurgeons who could do this were far and few between.
00:19:57
Speaker
The original lobotomy is not what you are probably thinking in your brain.
00:20:01
Speaker
It used to be two holes being drilled through your skull and, like, severing this part of
00:20:07
Speaker
of your brain between your frontal lobe connecting to the rest of your brain.
00:20:13
Speaker
They felt like psychosis and what have you was issues with the personality.
00:20:18
Speaker
All your hallucinations and stuff must live there.
00:20:20
Speaker
So they figured that if you could sever the tie between your frontal lobe and the rest of your brain, you won't be receiving those messages anymore.
00:20:26
Speaker
And they thought that that was true since people weren't experiencing those things anymore.
00:20:32
Speaker
They lost so much.
00:20:34
Speaker
They streamlined the process by, instead of drilling holes in the skull, by accessing the brain through the eye socket with an eye.
00:20:43
Speaker
Skip this part if you don't want to hear the descriptions of it.
00:20:46
Speaker
I mean, it's not that graphic.
00:20:49
Speaker
But if you have a hypergraphic brain.
00:20:52
Speaker
Visual, yeah, maybe skip.
00:20:54
Speaker
For the next minute.
00:20:57
Speaker
It's not that bad.
00:21:03
Speaker
Oh, like eye stuff.
00:21:04
Speaker
If you're squirmish, you can move fast forward just a second.
00:21:10
Speaker
You already heard it.
00:21:12
Speaker
But basically, you know, they take what looks like an ice pick and then they access your brain through your eye socket.
00:21:20
Speaker
They have like a little mallet that they use and then it's like a quick boop, boop, boop.
00:21:27
Speaker
The lobotomy is done.
00:21:29
Speaker
And so because they simplified this process so much, they were able to train a ton of people on it, and they were able to just roll them the fuck out.
00:21:39
Speaker
And people were getting lobotomies left and right, man.
00:21:42
Speaker
After World War II, there's another...
00:21:47
Speaker
obviously, in psych patients coming into facilities because war creates an outrageous amount of trauma.
00:21:55
Speaker
This parallels the time where over 200,000 people who were institutionalized in Germany were murdered in Nazi Germany.
00:22:04
Speaker
And actually, this was a precursor, this documentary said this was a precursor to the targeting of all disabled folks and then Jewish people.
00:22:12
Speaker
So, like, it started...
00:22:14
Speaker
with this idea that they were getting rid of all of these people who were a burden to society.
00:22:22
Speaker
And then that was translated into whoever they wanted to target next.
00:22:26
Speaker
Right, right, right.
00:22:28
Speaker
coming back to the United States.
00:22:30
Speaker
The idea that these were curative places is crushed.
00:22:32
Speaker
Now we're like, now people are like, these are hell holes that warehouse people.
00:22:37
Speaker
And this really like, I think, impose a sense of urgency on doctors to make use of the medical advancements that were suggested by the lobotomy.
00:22:47
Speaker
Bitches still don't know what's going on with the brain, but they do start observing people with brain injuries and conclude that the damage to the frontal lobe altered personality and behavior.
00:22:56
Speaker
Which is where the belief comes from that all of your stuff was just kind of housed there.
00:23:00
Speaker
And they were like, if we could sever the frontal lobe and change people in such a drastic way, maybe we can make asylums obsolete.
00:23:09
Speaker
And they thought that they could disrupt mental illness in general by offering this singular cure.
00:23:16
Speaker
That is absolutely wild.
00:23:20
Speaker
Then we're leading into like pharmaceutical discoveries.
00:23:23
Speaker
The first antipsychotic was discovered on accident.
00:23:25
Speaker
It was used to treat another illness.
00:23:27
Speaker
And then they noticed the drug calmed the patients down.
00:23:29
Speaker
Thorazine was one of these.
00:23:31
Speaker
It was coined the chemical lobotomy.
00:23:33
Speaker
And so they were giving people these antipsychotics that they claimed worked as a lobotomy and patients were just discharged from hospital.
00:23:41
Speaker
So for the first time, people are being discharged from hospitals en masse for the first time in, I don't know, decades.
00:23:48
Speaker
or since the inception of asylums.
00:23:50
Speaker
And they felt like this was a success.
00:23:52
Speaker
And obviously this had very harmful side effects, but it allowed for the immediate release of
00:23:58
Speaker
from the psych institution.
00:23:59
Speaker
So they said, we've done our job, which I think is a theme in general, right?
00:24:04
Speaker
Like they're like, I see the immediate result of this and I assume that the result is positive.
00:24:08
Speaker
Therefore I'm not going to take any ownership for the long-term impacts of whatever this is.
00:24:13
Speaker
Right, right, right.
00:24:14
Speaker
I mean, that's where they landed.
00:24:15
Speaker
And then the pharmaceutical company industry is kind of born through this legacy of lobotomizing patients.
00:24:31
Speaker
I found this in a book written by Janelle Johnson about the American lobotomy.
00:24:36
Speaker
She talks about a place called Lackin, which was a tiny unincorporated community on the border between West Virginia and Ohio.
00:24:46
Speaker
There was a small hospital that housed the state's African American patients.
00:24:51
Speaker
So you asked a question about
00:24:52
Speaker
how Jim Crow era kind of intersected with this, and this is talking about that.
00:24:57
Speaker
She talks about the conditions of Black Kin being awful, poor toilet facilities, inadequate staffing, no therapy, crowded dormitories, mingling of children and adults in the same wards.
00:25:09
Speaker
As a Black institution in Jim Crow era, she says,
00:25:13
Speaker
Lackin faced a number of additional hardships.
00:25:15
Speaker
One was the stark difference with regard to the appropriation of state funds.
00:25:20
Speaker
In white institutions like Weston, attendants were paid $90 a month.
00:25:24
Speaker
At Lackin, the African-American attendants were paid $75 a month.
00:25:28
Speaker
In addition, although Weston State Hospital had separate buildings in which patients with tuberculosis were housed, Lackin's patients with tuberculosis lived with others.
00:25:37
Speaker
And there was no preventative measures taken to stop the spread of disease.
00:25:41
Speaker
So clearly there were inequalities, which is not surprising.
00:25:46
Speaker
The conditions were horrific and then they were more horrific.
00:25:49
Speaker
Yeah, they were more horrific here.
00:25:51
Speaker
So she's talking about an exposé that was written by someone named Armin Trout.
00:25:56
Speaker
She talks about how he, in this exposé, doesn't give a comment or critique on this racial inequality and that he just relies on the trope of the dangerous mental patient to make the argument that funding Weston was a matter of public safety.
00:26:12
Speaker
and he employed racial fear in order to make his case for reform at Lackin.
00:26:17
Speaker
She says, weaving stereotypes about race and mental illness, the Lackin story is entitled, Escape is Easy at Lackin for Mentally Ill, and then uses that word.
00:26:28
Speaker
So this expose was ran at the same time as the Snake Pit,
00:26:35
Speaker
which electrified audiences with its shocking picture of miseries of hospital life.
00:26:40
Speaker
So I wanted to share that, that there was also a hospital existing nearby outside of Weston.
00:26:47
Speaker
In 1950, Lackin superintendent invited Walter Freeman to demonstrate the procedure of ice-wick lobotomy for hospital staff.
00:26:56
Speaker
Impressed by what they saw, the Board of Controlled commissioned Freeman to begin a project of what can only be described as the nation's first and only attempt at surgical deinstitutionalization.
00:27:06
Speaker
And so that is the West Virginia Lobotomy Project, which began in the summer of 1952.
00:27:11
Speaker
And Walter Freeman operated upon 228 patients in the hospitals of Blacken, Huntington, Spencer, and Weston.
00:27:20
Speaker
So I'm going to talk a little bit about historical context around this time.
00:27:28
Speaker
In 1946, there was a Life magazine exposé actually called Bedlam that was exposing the really bad stuff that was happening at asylums across the nation.
00:27:40
Speaker
And it was one of the first featured articles that critiqued the quality of mental health institutions in America.
00:27:47
Speaker
And actually during World War II, many of what were called conscientious objectors who did not want to fight in the war were assigned to work at institutions.
00:27:57
Speaker
And so they were able to see what the quality of life was like there.
00:28:02
Speaker
And a lot of articles and exposés came out after these people were...
00:28:06
Speaker
offered insight into what these places actually look like.
00:28:08
Speaker
And then in July of 1946, President Harry Truman signed the National Mental Health Act, calling for a National Institute of Mental Health to conduct research into the mind, brain and behavior and reduce mental illness.
00:28:23
Speaker
That was its purpose.
00:28:25
Speaker
And so the National Institute of Mental Health, which is still like today, was formed in
00:28:30
Speaker
Then, formally established in April of 1949, the act was supposed to make the mental health of folks a federal priority and was inspired by the poor mental health of veterans and their families after the World Wars.
00:28:43
Speaker
Through the National Mental Health Act, a new form of diagnosis and treatment was created to better help those face mental health problems.
00:28:51
Speaker
And it was discovered during this time that mental health patients benefited from evaluation and treatment rather than being institutionalized.
00:28:58
Speaker
And the act started to redirect financing from the state level to a national level and placed the National Institute of Mental Health for further research and analysis on brain and psychiatric disorders.
00:29:09
Speaker
Going back just a little bit to talk about like diagnoses and the history of the DSM or the Diagnostic Statistical Manual.
00:29:21
Speaker
The use of institutions for the insane was created.
00:29:25
Speaker
That was kind of the precursor to the DSM.
00:29:28
Speaker
This publication was revised up to 10 times up till 1942.
00:29:32
Speaker
And at this time, it had really broad categories and Freudian psychiatry was predominant at this time.
00:29:37
Speaker
And this was kind of present in the statistical manual.
00:29:40
Speaker
There was a need to develop a classification system that was more universal because there were many different diagnoses like we already were talking about and diagnostic systems that were present.
00:29:51
Speaker
And so in 1952, the DSM-1 was released.
00:29:55
Speaker
And this was also after a series of successful antipsychotic drugs were introduced that don't cure psychosis, but control its symptoms.
00:30:05
Speaker
So the first of these was actually called Thorazine or Thorazine.
00:30:09
Speaker
chlorpromazine, which is still used today, and it was discovered to help with hallucinations and delusions.
00:30:16
Speaker
The chemical lobotomy.
00:30:19
Speaker
So it was around the same time, which is connected, so keep in mind that these drugs are being produced around the same time that a universal classification system is needed, and the DSM-1 is released in 1952.
00:30:34
Speaker
It had 102 broad diagnostic categories and
00:30:39
Speaker
Also based on psychodynamic or Freudian principles, the two main groups were conditions that were assumed to be caused by some type of brain dysfunction and conditions that were assumed to be the result of the effects of environmental stress.
00:30:52
Speaker
So like nature versus nurture conditions.
00:30:54
Speaker
So the first is nature, second is nurture.
00:30:57
Speaker
And the second one is about people's inability to adapt to those environmental stressors.
00:31:03
Speaker
And the second group was subdivided into psychoses, which is like schizophrenia and other psychotic disorders and psychoneuroses like depression, personality disorders, anxiety, which is where the term like neurotic.
00:31:17
Speaker
comes from for people with anxiety.
00:31:20
Speaker
Despite the development of this manual, people didn't really use it that much and it had not much impact on the actual diagnostic process.
00:31:29
Speaker
And this, you know, kind of lack of use set the stage for the development of a second edition, which also, you know, most psychiatrists ignored.
00:31:39
Speaker
And I'll come back to this, but 1951, the National Association of Mental Health was also formed.
00:31:45
Speaker
And like I said earlier, it was in the 1950s where the number of people in the hospitals across the country is peaking.
00:31:52
Speaker
Estimated around 560,000 people were institutionalized across the country.
00:31:57
Speaker
And it was also around this time that behavior therapy is starting to be developed first with people with phobias.
00:32:04
Speaker
And they're like, oh, people with phobias can actually recover and like not have this phobia anymore through the use of behavior therapy.
00:32:10
Speaker
And so this is around the time where... They said, overwhelm and traumatize these people until they're not scared anymore.
00:32:20
Speaker
But this is also around the time where the first wave of deinstitutionalization occurs.
00:32:26
Speaker
And the Joint Commission on Mental Health and Health was authorized to investigate problems related...
00:32:32
Speaker
to the mentally ill.
00:32:34
Speaker
So connecting back to the lobotomies, President John F. Kennedy had a special connection to this because his sister, Rosemary,
Dr. Bateman: A Pioneer in Mental Health Care
00:32:42
Speaker
had been lobotomized at age 23 at the request of her father.
00:32:46
Speaker
And after his inauguration, Kennedy appointed a special president's panel of mental retardation is what it was called.
00:32:53
Speaker
And it included professionals and leaders of
00:32:56
Speaker
of the organization and in 1962 this panel published a report with 112 recommendations to better serve the mentally ill.
00:33:03
Speaker
So what else was happening around- It was assassinated two weeks later.
00:33:09
Speaker
I wonder if that was a part of the motivation.
00:33:13
Speaker
So at Weston State Hospital-
00:33:15
Speaker
Connected to what was going on in West Virginia during the same time, in the early 1960s, Dr. Mildred Bateman brought a change, and she was the director of the Department of Mental Health from 1962 to 1977 in West Virginia.
00:33:32
Speaker
The first black woman to hold a high administrative position in government.
00:33:38
Speaker
And she was, I'm reading off of this website, which is Marshall University School of Medicine, remembering the legacy of Dr. Mildred Mitchell Bateman.
00:33:47
Speaker
She was also the first woman to hold that position.
00:33:51
Speaker
She made a lot of really positive contributions to the field of mental health, which connects to Weston because she was the superintendent at Lackin State Hospital, which I just mentioned.
00:34:03
Speaker
And she developed innovative programs for patients.
00:34:05
Speaker
deemed hopeless and promoted treatments with psychosocial rehabilitation.
00:34:10
Speaker
And then in 1962, she was the first African-American woman to run a state department.
00:34:15
Speaker
And she served as the director of West Virginia's Department of Mental Health.
00:34:20
Speaker
And she began a number of programs to advance the care of West Virginia's mentally ill.
00:34:25
Speaker
And in 1973, she was the first African-American woman to hold office in the American Psychiatric Association, also known as the APA.
00:34:33
Speaker
And she served as the vice president.
00:34:36
Speaker
One quote from Dr. Mildred Mitchell Bateman is that she said, no one has a right to decide that patients aren't going to get any better.
00:34:45
Speaker
She spent a lot of her career advocating for the mentally ill, and she was part of the deinstitutionalized process.
00:34:54
Speaker
She actually later received a Lifetime Achievement Award from the American Psychiatric Association in 2000.
00:35:00
Speaker
And she passed away in 2012 at the age of 89.
00:35:05
Speaker
She was well known as an exceptional teacher and sought to teach others to treat psychiatric patients with respect and dignity.
00:35:12
Speaker
She has also been described as humble, tireless, and a passionate advocate for those with psychiatric disorders.
00:35:18
Speaker
She was directly connected to the deinstitutionalized process that happened at Weston State Hospital starting in the 1960s because she was the director of the Department of Mental Health in Broadway.
00:35:32
Speaker
Shoutouts to Dr. Mildred Bateman.
00:35:36
Speaker
So around this time, there's like more critiques on asylums coming out.
00:35:41
Speaker
There is a book that comes out by a psychiatrist called The Myth of Mental Illness that argues that there's no such thing as schizophrenia.
00:35:50
Speaker
And there's just critiques about people having symptoms of psychosis as a direct result of being in these institutions.
00:35:59
Speaker
Say more about no such thing as schizophrenia.
00:36:01
Speaker
I mean, is it just an argument that what we call mental illness is just a rational response to the conditions that we live in?
00:36:12
Speaker
I know that there was a person who was advocating for something similar saying that like the DSM would be pretty much nothing if we adequately accounted for trauma and the impact of it.
00:36:21
Speaker
Okay, so what he meant by that is that he's not denying the existence of these conditions or the suffering or distress that people experience.
00:36:30
Speaker
So either he's saying that these conditions shouldn't be classified as medical diseases, like physical diseases are classified.
00:36:37
Speaker
He's pretty much saying like the disease in the mind is impossible in the way that a physical disease shows up.
00:36:44
Speaker
So what this book was saying was kind of going against the disease model of mental illness.
00:36:49
Speaker
I don't think he was providing another option for it.
00:36:52
Speaker
He was just saying this can't be classified in the same way as physical illnesses are, which is fair, especially given how little they knew about the brain at this time.
00:37:02
Speaker
But the person that said that people in institutions were exhibiting psychotic symptoms because of being institutionalized was named Goffman, and he was another critic of the mental health establishment.
00:37:13
Speaker
And then connecting this back to the MKUltra series, in 1962, counterculture author Ken Kesey writes the novel One Flew Over the Cuckoo's Nest, which is based on his experiences working in the Psychiatric Board of the Veterans Administration.
00:37:28
Speaker
He is motivated by seeing that his patients don't really have mental illnesses.
00:37:34
Speaker
They simply behave in ways of rigid societies and unwilling to accept.
00:37:38
Speaker
And so that's what his book is a critique on.
00:37:41
Speaker
And then it was made into a play and into a movie that has Jack Nicholson.
00:37:46
Speaker
And so there's a lot of media kind of coming out that's going against the norm at the time of mental health and changes are happening and reform is happening.
00:37:57
Speaker
And this kind of leads to the wave of deinstitutionalization that occurs right after this.
00:38:03
Speaker
So also in the mid-1960s, the psychiatric survivors movement or consumer or ex-patient movement begins.
00:38:11
Speaker
This emerged from social unrest and the civil rights movement among people who had experienced human rights violations in the mental health care system.
00:38:20
Speaker
And the movement calls attention to the need for self-determination for users of mental health services and
00:38:27
Speaker
supports advocates in uniting under the banner of, quote, mad pride to affirm their personhood.
00:38:33
Speaker
So people kind of like, standing up for themselves saying what happened to them was not okay.
00:38:40
Speaker
And this is around the same time as many people who are mentally ill are removed from institutions.
00:38:46
Speaker
and are directed towards local mental health homes and facilities.
00:38:50
Speaker
And actually, it will drop from the peak of 560,000 to just about over 130,000 in 1980.
00:38:55
Speaker
In 1963, the passage of the mental retardation facilities and community mental health facilities
00:39:06
Speaker
Centers Construction Act, which is now just the Community Mental Health Act, provides a first federal money for developing a network of community-based mental health services.
00:39:16
Speaker
So kind of shifting to more of an outpatient model of care and advocates for deinstitutionalization, talk about how people with mental illness will voluntarily seek out treatment at these facilities if they need it.
00:39:28
Speaker
And there's also the existence of partial hospitalization programs and intensive outpatient programs.
00:39:36
Speaker
As this connects to Weston State, community mental health centers pop up around 1962, 1963.
00:39:42
Speaker
The state wrote a plan for these mental health programs and funds for state hospitals were shifted towards community mental health centers.
00:39:49
Speaker
And 47 community mental health programs began in West Virginia after this act was passed.
00:39:56
Speaker
In the 70s, the psychiatric survivors formed a group called the Liberation of Mental Patients, and they also formed the National Alliance on Mental Illness, which still exists now today.
00:40:09
Speaker
They felt the need to challenge the system's treatment of the mentally ill, and they targeted issues around involuntary commitment, the use of electroshock therapy, anti-psychotic medication, and coercive psychiatry.
00:40:23
Speaker
And many of these groups were successful in the judiciary system.
00:40:27
Speaker
In 1975, the Court of Appeals ruled in favor of the Mental Patients Liberation Front, establishing the right of a patient to refuse treatment if they wanted to.
00:40:39
Speaker
Yeah, so a lot of shifts taking place, and NAMI is also lobbying to improve mental health services and gain the quality of insurance coverage for mental illness.
Controversies Surrounding the DSM
00:40:52
Speaker
kind of shifting back to talking about the DSM now, in the 1980s is when the third edition of the DSM became available, and it was the first edition of the DSM that led to the APA's, what's known as commercial success.
00:41:09
Speaker
I read an article called Towards Decolonizing Diagnosis, a Critical Review and Suggested Alternatives, written by Krista M. Mallett, Shani Barclough, and Terence Yee.
00:41:21
Speaker
And it talks about how the DSM is embedded into the healthcare system in the U.S. in a way that all mental health professionals, from counselors to social workers,
00:41:30
Speaker
must assign clients a DSM diagnosis in order to receive reimbursement for their services.
00:41:36
Speaker
She talks about how there's a conflict of interest affiliated with the DSM in regard to the instruments' ties to the pharmaceutical industry.
00:41:47
Speaker
69% of the DSM-5 task force, which is one of the most recent DSMs to come out, were directly affiliated with the pharmaceutical industry.
00:41:54
Speaker
And I feel like that is connected to how the DSM was created just around the time that a lot of psychiatric drugs were being put on the market as well.
00:42:04
Speaker
And there was a commercialization of psychiatry in a way that hadn't existed before.
00:42:11
Speaker
And it shifted from asylums to outpatient care.
00:42:14
Speaker
But then there was the establishment of like the Mental Health Act, but also the APA and all these other organizations that had ties to the pharmaceutical industry.
00:42:24
Speaker
And it still kind of exists today.
00:42:26
Speaker
So in the review of the DSM, A History of Psychiatry's Bible, they talk about biometrician and psychiatrist Robert Spritzer, who led the APA's task force and helped to secure the manual's professional and popular acceptance through strategic compromises.
00:42:43
Speaker
However, 40 years later today, this, you know,
00:42:48
Speaker
Manual has failed to deliver on its promises for better explanations and better treatments for mental illnesses and still has a lot of controversy associated with it.
00:42:59
Speaker
Scholar L. Johnston notes that the most damaging effect of diagnostic labels is to obscure people's personal meanings, conceal their stories, and sever the link between their distress and the circumstances of their lives.
00:43:12
Speaker
Such distress is often related to contextual experiences of trauma when erroneously diagnosed as individual dysfunction blames the client rather than societal injustices.
00:43:25
Speaker
This, in essence, is pathologizing the assumption that because individuals exhibit certain set of symptoms, they are themselves disordered.
00:43:33
Speaker
So just talking about how the DSM puts the onus and blame and pathologizes an individual for having super normal reactions to the conditions that they're living in and then
00:43:46
Speaker
takes attention away from actually changing those conditions and trying to quote fix the individual, you know, which is super tied to what asylums were trying to do as well.
00:43:56
Speaker
It's very Kirkbride.
00:43:58
Speaker
Just like same thing, different font.
00:44:02
Speaker
And, you know, the DSM is still very much used today and is, you know, psychiatry's Bible.
00:44:08
Speaker
And even in the latest...
00:44:11
Speaker
version of the DSM, which is DSM-5TR.
00:44:14
Speaker
There was efforts to diversify input, but, you know, there was no notes about whether clients or, like, counselors were actually included with input in creating this.
00:44:26
Speaker
Lots of the stuff that existed within the DSM remained...
00:44:29
Speaker
unchanged, the stuff that had controversy associated with it.
00:44:32
Speaker
And then they just created new pathologies like prolonged grief disorder and unspecified mood disorder, which like just continue to pathologize individuals rather than addressing.
00:44:44
Speaker
the social conditions in which we exist right now that might be leading to prolonged grief disorder and unspecified mood disorders.
00:44:53
Speaker
And the DSM is also a US manual and other countries in the world use the ICD, which includes complex trauma and complex PTSD in it, but for some reason
00:45:03
Speaker
The DSM does not want to include that within its diagnostic criteria, probably because of a lot of the mental illnesses and disorders that exist within the DSM would then be collapsed under complex trauma and under complex PTSD, which makes things complicated when it comes to insurance and prescribing pharmaceuticals and things like that.
00:45:26
Speaker
This article goes on to talk about alternatives to the DSM, which I'm not going to go into right now.
00:45:32
Speaker
But if you're curious, you can always look into it.
00:45:35
Speaker
And I will share one last quote.
00:45:37
Speaker
Mental health counseling is a profoundly political experience, as asserted by self-described decolonizing therapist Mullen.
Principles of Disability Justice
00:45:46
Speaker
We cannot heal drinking from a poisoned river.
00:45:49
Speaker
A multitude of stakeholders across the globe, from scholars to practitioners to clients receiving mental health services, are fighting to redress that poison.
00:45:58
Speaker
In spite of these efforts, the current DSM system remains entrenched, reifying the status quo as a consequence, failing and at times harming clientele.
00:46:08
Speaker
so just interesting to learn about that as it parallels asylums because it is something that comes after asylums were a thing as a way to kind of improve the state of mental health care but then is replicating the same forms of control just in a different way we're not learning where's the learning well I mean
00:46:36
Speaker
They're acting like Kirkbride's model exists in a vacuum, you know, like this is just happening within the confines of this guy's vision and the people who kind of circled around him not realizing like, oh, actually, maybe he is a product.
00:46:51
Speaker
of our society and is very much mirroring our- like was able to leverage what we know to be true, our values, our individualism, our capitalism, and putting it onto a system that ended up being deeply dehumanizing.
00:47:08
Speaker
And it would make sense that we would replicate those same structures in a different way because that's who we are.
00:47:14
Speaker
But especially when we're still living under systems that are inherently oppressive and traumatizing, like that's the reason that a lot of people struggle with mental health in the first place.
00:47:25
Speaker
So we're not going to be, you know, changing the or, you know, living in a different system that isn't capitalism and living in a different system that isn't upheld by white supremacy.
00:47:36
Speaker
then we're still going to have these same people experiencing these same issues.
00:47:41
Speaker
And there's not an addressing really of that connection between oppression and mental health.
00:47:48
Speaker
By the large majority within the field of mental health, it's still very much an individual pathologizing framework.
00:47:57
Speaker
And even, you know, as someone that's a therapist, like, I feel like I have to have intentional conversations with my clients about diagnosis, because especially if it's someone who I see who is using insurance, like, you have to provide a diagnosis for insurance.
00:48:13
Speaker
And it's important to have a critical understanding.
00:48:16
Speaker
understanding of what that actually means and you know just because you have a certain diagnosis that doesn't make it who you are as a person and a lot of people do internalized you know if i have depression that means i'm a depressed person all of the time um or like you know because i have this mental health diagnosis that means that something is wrong with me right
00:48:38
Speaker
Versus like this is a super normal reaction to your body just surviving under the conditions that it's in.
00:48:45
Speaker
And that depression is actually a shutting down of your nervous system because it's overwhelmed by the stress that it's under.
00:48:53
Speaker
And I want to acknowledge that like I think that diagnoses are helpful in a lot of ways or they can be.
00:49:02
Speaker
In that we are able to then have a framework for the what's going on and the why something might be going on.
00:49:09
Speaker
And then you're able to be like, oh...
00:49:12
Speaker
actually, I'm not inherently a lazy person.
00:49:14
Speaker
I'm experiencing these things.
00:49:16
Speaker
And then you can learn to figure out what it is that you need in your patterns.
00:49:22
Speaker
And, you know, I think it can be helpful in that way.
00:49:24
Speaker
And so I guess it's just like, it's not to take away from the benefits of having a name to describe your experience and therefore understand yourself better.
00:49:35
Speaker
Right, right, right.
00:49:37
Speaker
I totally agree with that as well.
00:49:39
Speaker
At the end of the day, diagnoses are categories of symptoms that help you understand yourself better and potentially meet your needs better, whether that be with therapy, medication, or other forms of healing that exist as well, or just trying to change the environment that you live in.
00:49:55
Speaker
There's a lot of different ways to address diagnoses and categories of symptoms that are outside of the classical mental health care system.
00:50:11
Speaker
So 1980s, the population at Weston State Hospital is lower to a thousand.
00:50:17
Speaker
And there is a nationwide trend towards deinstitutionalization and medications are the main mode of treatment for mental health.
00:50:25
Speaker
But even in the 1980s, the hospital was still short-staffed with 20 nurses, four on the evening shift, and one on the night shift.
00:50:33
Speaker
Most important of the employees were the attendants or aides, and they were not well paid.
00:50:39
Speaker
The average pay in the 1990s was about $16,000 a year for all employees.
00:50:46
Speaker
Even though physicians made $60,000 to $70,000 a year, the average was still $16,000 a year.
00:50:52
Speaker
for the other employees.
00:50:54
Speaker
And a quarter of the staff were eligible for food stamps, even though they were doing tons of both physical and emotional labor.
00:51:02
Speaker
In the 70s and 80s, very interestingly, most of the physicians in the hospital were Asian.
00:51:08
Speaker
And I found this in that thesis that I read.
00:51:11
Speaker
She writes, many of these foreign physicians had heavy accents and were difficult to understand, and the nurses learned to understand them and acted as interpreters to the aides and patients.
00:51:22
Speaker
Miss Mason, the registered nurse, remembered there was an Indian doctor there when I first started and we had trouble with the patient.
00:51:29
Speaker
So I called her and she said, well, give him.
00:51:32
Speaker
And then it says Valium, but it's like written in a like way that it's like an accent that she didn't understand.
00:51:38
Speaker
And she said, doctor, I'm sorry, I don't understand you.
00:51:42
Speaker
And then she got mad at the nurse and spelled it out.
00:51:46
Speaker
And the nurse was like, oh, you mean Valium.
00:51:49
Speaker
But she couldn't understand her.
00:51:51
Speaker
White people are so dramatic because the way that... What do you think that it is?
00:51:54
Speaker
How many medications exist that sound anything like that?
00:51:58
Speaker
It can't be that different.
00:51:59
Speaker
The way that I'd be out in public with my grandma growing up and people would look at me and be like, what did she say?
00:52:07
Speaker
As if I'm translating for her when she's speaking English.
00:52:10
Speaker
She's speaking English.
00:52:12
Speaker
Yeah, so that was something that was included in the thesis, which I found interesting, especially given, you know, what we...
00:52:20
Speaker
know who was the hospital built for.
00:52:23
Speaker
It was for white people.
00:52:23
Speaker
So it's interesting that in the 70s and 80s, most of the physicians that were there were Asian.
00:52:28
Speaker
How had that happened?
00:52:30
Speaker
She didn't really talk about why that happened.
00:52:33
Speaker
She just included an arbitrary story about a mispronunciation and provided no context?
00:52:41
Speaker
I'm pretty sure she did.
00:52:42
Speaker
I, like, kind of scanned it.
00:52:45
Speaker
I don't understand.
00:52:48
Speaker
I bet you this is in alignment with...
00:52:52
Speaker
different tiers of immigration policies.
00:52:57
Speaker
That then there was a shift, right?
00:52:59
Speaker
It allowed people of a certain educational background to immigrate, which is why it was like doctors.
00:53:06
Speaker
I imagine that certain places were more likely to take foreign...
00:53:11
Speaker
Physicians, probably because they could pay less.
00:53:15
Speaker
Honestly, that's all it says.
00:53:17
Speaker
She doesn't say anything about why, you know, most of the doctors were from Asian nations.
00:53:23
Speaker
It says the physicians at the hospital through the 1970s and 80s were almost entirely foreign.
00:53:28
Speaker
But I feel like it's probably because of what you said in terms of being able to pay...
00:53:32
Speaker
foreigners less, most from Asian nations.
00:53:35
Speaker
This is where the model minority myth originated, right?
00:53:39
Speaker
In the 80s, there started being a lot more propaganda around that.
00:53:42
Speaker
Yeah, there isn't really a critical analysis
00:53:46
Speaker
of why that is in her thesis, which is disappointing.
00:53:51
Speaker
But in the 1990s, Weston State Hospital was designated as a National Historic Landmark, and in the last few years of the hospital's existence as a hospital, there was lots more just court-ordered patients, because most had been released from the hospital and were...
00:54:10
Speaker
receiving care elsewhere, but also theoretically these patients were being released and they were receiving care from outpatient facilities.
00:54:19
Speaker
But many of these mental health centers didn't have enough resources.
00:54:24
Speaker
And so often it wasn't followed up with if a patient didn't make the follow-up appointment after leaving.
00:54:29
Speaker
And many of them were lost through the cracks and ended up either houseless or incarcerated in prisons and jails.
00:54:38
Speaker
As we know, a lot of people in prisons and jails are mentally ill themselves.
00:54:43
Speaker
And that was one of the other repercussions of deinstitutionalization that people just ended up being reincarcerated, but in a different system.
00:54:52
Speaker
In 1994, only 224 patients died.
00:54:58
Speaker
which I think is interesting because that's much closer to the number that it was supposed to be at the whole time, 250.
00:55:05
Speaker
But it was a decrease of 96%, which is the largest in the nation amongst asylums.
00:55:11
Speaker
And the hospital was closed and another smaller hospital was built called the William R. Sharp Jr. Hospital.
00:55:18
Speaker
And the rest of the patients were transferred to that hospital.
00:55:22
Speaker
They didn't want to renovate Weston State, which is why they transferred them to the smaller hospital.
00:55:27
Speaker
to leave the building abandoned for a number of years, and many areas in the building were then damaged and vandalized.
00:55:33
Speaker
Since six years later in 2000, the Weston Hospital Revitalization Committee came together to maintain the history of the property.
00:55:42
Speaker
And then in 2007, Joe Jordan bought the building for $1.5 million at an auction with the intention of preserving and restoring it.
00:55:53
Speaker
It exists as a museum and historical site and ghost tours are offered.
00:55:58
Speaker
And Rebecca Gleason, or Rebecca Jordan, as you mentioned before, is his daughter, who's now the operations manager at this place.
00:56:06
Speaker
In 2007, the Trans-Allegheny Lunatic Asylum was again open to the public.
00:56:16
Speaker
And it was criticized by mental health advocates of the time saying,
00:56:20
Speaker
because it was exploiting the experiences of people with mental illness, especially because they used the term lunatic in the name.
00:56:27
Speaker
They also had events titled Psychopath and Lobotomy Flashlight Tour.
00:56:38
Speaker
And they stated that the reason that they used the name was because it was its original name.
00:56:43
Speaker
But I think that they did it for the shock value, because if you actually cared about being respectful, you could just call it like Weston State Memorial or something like that, you know?
00:56:54
Speaker
So areas can be toured, investigated.
00:56:57
Speaker
are the operating room, apartments, and the morgue.
00:57:00
Speaker
The main building of the asylum, also known as Kirkbride, holds several rooms that serve as a museum and it's located on the first floor.
00:57:09
Speaker
There are paintings, poems, and drawings made by patients in the art therapy programs.
00:57:15
Speaker
a room dedicated to the different medical treatments and restraints that were used in the past, and artifacts such as a straitjacket and hydrotherapy tub.
00:57:24
Speaker
They have a variety of tours, 45 to 90 minute heritage tours, which are about the history, photography tours, and then ghost hunts and tours of the farm cemeteries and awards for the quote, criminally insane.
00:57:38
Speaker
They also have events throughout the year, some of which I'll share, including a drag show,
00:57:47
Speaker
Not Shady Lady Productions presents Sadie Spears and the Trans-Allegheny Lunatic Asylum are proud to bring back another Shady Lady production.
00:57:58
Speaker
So, I don't know what is this queer capitalism that's going on here, but... I mean, there's a lot.
00:58:07
Speaker
Yeah, this is also in, like, West Virginia, which is, like, a pretty conservative state, but clearly...
00:58:13
Speaker
You know, whatever brings in the money.
00:58:15
Speaker
They're like pink washing.
00:58:21
Speaker
The shorter historical tour.
00:58:24
Speaker
Well, I also think that's such weird vibes because probably a lot of the people that were incarcerated at this institution were queer.
00:58:33
Speaker
And trans individuals.
00:58:37
Speaker
They have short historical tours that offer visitors to see the first floor of the Kirkbride, but they also have longer historical tours that allow visitors to see all four floors, apartments of the staff, the morgue, and the operating room.
00:58:49
Speaker
They also have two paranormal tours, both the start of sunset, a shorter one lasting two to three hours, and a longer one being the overnight option.
00:58:58
Speaker
And there's also an option for a private overnight tour that's just for you.
00:59:03
Speaker
Other events include the Asylum Ball, which takes place every October.
00:59:09
Speaker
And it's their annual costume party.
00:59:13
Speaker
Coming up this year, they have Father's Day Car Show.
00:59:21
Speaker
And then in October, they have a haunted house, flashlight tours, something called Hearst Mania, zombie paintball, and then the asylum ball, which I already mentioned.
00:59:30
Speaker
If I were a ghost, I'd be scratching bitches too.
00:59:33
Speaker
It's like, who cares?
00:59:35
Speaker
So I'm going to read some reviews.
00:59:37
Speaker
I want to say also, I'm not going to read them, but the people that run this place respond to a lot of the negative reviews.
00:59:47
Speaker
It has five stars and has over 7,000 reviews on TripAdvisors.
00:59:52
Speaker
So clearly, they do a good job of trying to maintain a serene image.
00:59:56
Speaker
Some of the reviews.
00:59:57
Speaker
Unfortunately, wasn't dragged into the depths of hell by a ghost, but our tour guide was pretty cool and I had an amazing time.
01:00:07
Speaker
Daddy Starbucks says, unbelievable time scared out of my mind.
01:00:12
Speaker
I don't want to explain it all for fear of paranormal bullying.
01:00:15
Speaker
Anyway, if you haven't gone, you must do yourself a favor and ask for Valerie and Brandy, the two baddest paranormal chicks on the planet, who will help you investigate more effectively because they know these spirits and the spirits know them.
01:00:30
Speaker
They are incredible hosts and even better investigators.
01:00:33
Speaker
Please bring a change of underwear.
01:00:36
Speaker
But then, one-star review.
01:00:39
Speaker
Disrespectful, historically and medically inaccurate.
01:00:42
Speaker
As a practicing psychiatrist, I was hoping to have a historically accurate and positive educational experience visiting an asylum that was in use for over 150 years.
01:00:51
Speaker
The medical, quote, facts...
01:00:54
Speaker
were inaccurate to say the least.
01:00:56
Speaker
The sign upon entry states celebrating 10 years of mental health education while a trip into the gift shop reveals ball caps with the saying, this hat covers my lobotomy scar.
01:01:09
Speaker
This is the epitome of disrespect for patients, providers, and institutions of mental health care.
01:01:15
Speaker
I should have known better than to visit a facility that prides itself on the quality of their ghost tours, but I had hopes there would be something worthwhile to see and learn today.
01:01:23
Speaker
This is a terrible mistake.
01:01:24
Speaker
If you're looking for a scary time, that's on you.
01:01:27
Speaker
But know that it's at the cost of enormous disrespect to the former patients of this facility.
01:01:34
Speaker
I mean, you should have known better.
01:01:36
Speaker
But they responded to this basically being like, this is standard across other museums that are asylums across the country to use dark humor to deal with what had happened in the past.
01:01:49
Speaker
Talking about the lobotomy jokes.
01:01:52
Speaker
There are a lot of standards that we seem to be adhering to.
01:01:57
Speaker
I mean, you used to host lobotomy flashlight tours, so I don't know what you expect from that.
01:02:02
Speaker
But, like, at least, like, this is what you're doing.
01:02:08
Speaker
Someone else said, went on two tours and I'd rather lit my money on fire and watched it burn.
01:02:17
Speaker
Sealing is falling in.
01:02:19
Speaker
Complete safety hazard in many areas.
01:02:22
Speaker
Someone could get injured badly or killed if a chunk of cement hit them just right.
01:02:26
Speaker
If you want to breathe in mold and mildew...
01:02:31
Speaker
Shayna does not like mildew.
01:02:33
Speaker
And risk your safety, then yes, this is the tour to take.
01:02:36
Speaker
I would not advise anyone to go on this tour or any other tour out there unless you want mold and mildew and disappointment in your life.
01:02:44
Speaker
Totally not worth money.
01:02:46
Speaker
If it was free, it would be too much money.
01:02:49
Speaker
Just because you'd be wasting your gas.
01:02:51
Speaker
The outside of the facility is cool to get pics of, but nothing more.
01:02:55
Speaker
Extremely disappointed and would not recommend.
01:02:58
Speaker
Trans Allegheny, you asked for the review.
01:03:01
Speaker
I stated nothing but complete facts.
01:03:05
Speaker
So two different bad reviews.
01:03:07
Speaker
One was trying to have a good time.
01:03:09
Speaker
And I was like, I'm impressed.
01:03:10
Speaker
And was feeling unsafe.
01:03:12
Speaker
And the other person was like, I'm a psychiatrist and this is super disrespectful.
01:03:19
Speaker
It makes sense that spirits are mad.
01:03:21
Speaker
We should leave an episode link.
01:03:25
Speaker
Yeah, we should put our episode on TripAdvisor.
01:03:28
Speaker
You should put our episode on TripAdvisor.
01:03:30
Speaker
Yes, you should put it.
01:03:31
Speaker
Someone should put it there.
01:03:33
Speaker
So that's the Westin State Hospital from start to finish.
01:03:37
Speaker
Still is open today.
01:03:39
Speaker
I wouldn't go there, but, you know.
01:03:42
Speaker
If you choose to go there, that's your prerogative.
01:03:44
Speaker
We wanted to end on something a little more positive.
01:03:48
Speaker
Not more positive, but just like highlight some work in the disability justice and disability rights movement tied to the mental health system.
01:03:58
Speaker
So, you know, you have fuckery like this still happening, but we also have people who have really been dedicating their whole lives and then putting their bodies on the line to advance disability justice.
01:04:10
Speaker
I wanted to highlight a piece of work done by Sins Invalid.
01:04:16
Speaker
It's a disability justice organization based in the Bay Area, and
01:04:21
Speaker
And they have a variety of programs, but this primer basically is a rundown for like what disability justice is and like varied perspectives on it.
01:04:32
Speaker
It also kind of takes you through at the beginning, the transition from disability rights into disability justice and the differentiation between that.
01:04:40
Speaker
It's really beautiful work.
01:04:42
Speaker
And I think that if
01:04:45
Speaker
you're somebody who is rooted in liberatory values, a disability justice framework, if you're not already invested in it, should be something that is central because it undergirds all other forms of justice work.
01:05:01
Speaker
And so I can put a link in the description.
01:05:05
Speaker
You can buy this primer for $7 online and you'd be donating to a worthy org.
01:05:12
Speaker
And it's disabled-led,
01:05:16
Speaker
They kind of start with like, okay, so we're moving into the next stage in movement evolution.
01:05:22
Speaker
Earlier you heard Akshi talking about what was essentially the disability rights movement.
01:05:28
Speaker
And, you know, they named there was phenomenal and historic work done by disabled people and allies to develop disability rights in the U.S.,
01:05:35
Speaker
and it had many successes in advancing a philosophy of independent living and opening possibilities for people with disabilities.
01:05:41
Speaker
The U.S. disability rights movement established civil rights for people with disabilities.
01:05:46
Speaker
Like other movements, the current disability rights movement includes advocacy organizations, service provision agencies, constituency-led centers, membership-based national organizations, as well as cultural and academic spaces.
01:05:59
Speaker
And like many movements, it's contextualized within its time and left us with cliffhangers.
01:06:04
Speaker
It's one strategy many needed to combat ableism.
01:06:08
Speaker
It's single issue, identity-based.
01:06:10
Speaker
Its leadership has historically centered white experiences.
01:06:13
Speaker
Its framework leaves out other forms of oppression and the ways in which
01:06:17
Speaker
privilege is leveraged at different times and for various purposes.
01:06:21
Speaker
At its core, it centers people who can achieve rights and access through a legal or rights-based framework, which we know is not possible for many disabled people or appropriate for all situations.
01:06:32
Speaker
And so disability rights movements was kind of like in parallel to like the mad pride of
01:06:39
Speaker
work that folks were doing and although there is significant overlap in its efforts they were kind of there were gaps there were gaps they were adjacent to one another and overall we see in social movements over and over that the movements that get to move forward are always white led and cis led and straight led and male led
01:07:01
Speaker
So this is kind of what they're naming.
01:07:24
Speaker
The root of disability oppression is ableism, and we must work to understand it, combat it, and create alternative practices rooted in justice.
01:07:32
Speaker
While a concrete and radical move forward towards justice for disabled people, the disability rights movement simultaneously invisiblized the lives of people who were lived at the intersecting junctures of oppression.
01:07:43
Speaker
Disabled people of color, immigrants with disabilities, queers with disabilities, trans and gender non-conforming people with disabilities, people with disabilities who are houseless, who are incarcerated, who have their ancestral lands stolen amongst others.
01:07:58
Speaker
In response to this, in 2005, disabled activists of color, originally queer women of color, incubated in progressive and radical movements that did not systematically address ableism, namely myself, who is Patty Burns.
01:08:14
Speaker
Patti Byrne, who I've actually... So when I did my 60-hour rape crisis training, she came in to talk about sexual violence in disabled communities and talked about supporting survivors through a disability justice lens, which is a whole other tangent.
01:08:30
Speaker
And Mia Mingus, soon to be joined by Leroy Moore...
01:08:33
Speaker
Stacey Milburn, Eli Clare, and Sebastian Margaret began discussing a second wave of disability rights and ultimately launched a framework that we called disability justice.
01:08:42
Speaker
Given the isolation enforced by ableism and classed boundaries, many of us have found ourselves as agents of change within respective communities and isolated from in-person community, while other disabled people of color or queer or gender non-conforming crips.
01:08:56
Speaker
Many of us have found liberated zones that we celebrate our multiple identities online instead.
01:09:01
Speaker
In many ways, disability justice is a developing framework that some call a movement.
01:09:05
Speaker
We're still identifying the we.
01:09:07
Speaker
Disability justice activists, organizers, and cultural workers understand that able-bodied supremacy has been formed in relation to other systems of domination and exploitation.
01:09:17
Speaker
The histories of white supremacy and ableism are inextricably entwined, both forged in the crucible of colonial conquest and capitalist domination.
01:09:26
Speaker
One cannot look at the history of US slavery, the stealing of indigenous lands, and US imperialism without seeing the way that white supremacy leverages ableism to create a subjugated other that is deemed less worthy, abled, smart, capable.
01:09:39
Speaker
A single issue civil rights framework is not enough to comprehend the full extent of ableism and how it operates in society.
01:09:47
Speaker
We cannot comprehend ableism without grasping its interrelations with heteropatriarchy, white supremacy, colonialism, and capitalism.
01:09:55
Speaker
Each system benefits from extracting profits and status from the subjugated quote-unquote other.
01:10:01
Speaker
500 plus years of violence against black and brown communities includes 500 plus years of bodies and minds being deemed dangerous by being non-normative, again not simply within able-bodied normativity,
01:10:12
Speaker
but within the violence of heteronormativity, white supremacy, and gender normativity, within which our various bodies and multiple communities have been deemed deviant, unproductive, and invalid.
01:10:23
Speaker
A disability justice framework understands that all bodies are unique and essential, that all bodies have strengths and needs that must be met.
01:10:31
Speaker
We know that our bodies are powerful, not despite of the complexities of our bodies, but because of them.
01:10:36
Speaker
We understand that all bodies are caught in the bindings of ability, race, gender, sexuality, class, nation-state, and imperialism, and that we cannot separate them.
01:10:45
Speaker
These are the positions from which we struggle.
01:10:47
Speaker
I'm going to pull one more thing from this and then pass it back to you to talk about Project Let's.
01:10:51
Speaker
There are 10 principles of disability justice that they highlight in grounding this work.
01:10:56
Speaker
So, one is intersectionality.
01:10:58
Speaker
We know that each person has multiple identities and that each identity can be a site of privilege or oppression.
01:11:03
Speaker
The mechanical workings of oppression and how it outputs shift depending on the characteristics of any given institutional or interpersonal interaction.
01:11:11
Speaker
Number two, they emphasize leadership of the most impacted.
01:11:15
Speaker
We know ableism exists in the context of other historical systemic oppressions.
01:11:19
Speaker
We know to truly have liberation, we must be led by those who know most about these systems and how they work.
01:11:25
Speaker
Number three is an anti-capitalist politic.
01:11:28
Speaker
We are anti-capitalists as the very nature of our minds and bodies often resist conforming to a capitalist normative level of production.
01:11:35
Speaker
We don't believe human worth is dependent on what and how much a person can produce.
01:11:39
Speaker
We critique a concept of labor as defined by able-bodied supremacy.
01:11:43
Speaker
We understand capitalism to be a system that promotes private wealth accumulation for some at the expense of others.
01:11:50
Speaker
Number four, cross-movement solidarity.
01:11:52
Speaker
Necessarily cross-movement.
01:11:54
Speaker
Disability justice shifts how social justice movements understand disability and contextualize ableism, lending itself toward a united front politic.
01:12:02
Speaker
Number five, recognizing wholeness.
01:12:05
Speaker
We value our people as they are for who they are and understand that people have inherent worth outside of capitalist notions of productivity.
01:12:12
Speaker
Each person is full of history and life experience.
01:12:16
Speaker
Number six, sustainability.
01:12:18
Speaker
We pace ourselves individually and collectively to be sustained long term.
01:12:22
Speaker
We value the teachings of our lives and bodies and understand that our embodied experience is a critical guide and reference pointing us toward justice and liberation.
01:12:31
Speaker
Number seven, commitment to cross-disability solidarity.
01:12:34
Speaker
We are committed to breaking down ableist, patriarchal, racist, classed, isolation between people with physical impairments, people who identify as sick or chronically ill, psych survivors, and those who identify as crazy, neurodiverse people, people with cognitive impairments, and people who are unwell.
01:12:48
Speaker
of a sensory minority, as we understand that isolation ultimately undermines collective liberation.
01:12:55
Speaker
Before the massive colonial project of Western European expansion, we understood the nature of interdependence within our communities.
01:13:02
Speaker
We attempt to meet each other's needs as we build towards liberation, without always reaching for state solutions, which inevitably then extend its control further over our lives.
01:13:13
Speaker
Collective Access As Black, brown, and queer crips, we bring flexibility and creative nuance to engage with each other.
01:13:21
Speaker
We create and explore new ways of doing things that go beyond able-bodied and minded normativity.
01:13:26
Speaker
Access needs aren't shameful.
01:13:28
Speaker
We all have various capacities which function differently in various environments.
01:13:33
Speaker
And number 10, collective liberation.
01:13:35
Speaker
How do we move together as people with mixed abilities, multiracial, multigendered, mixed class across the orientation spectrum where no body or mind is left behind?
01:13:45
Speaker
And then it talks about how disability justice honors the longstanding legacies of resilience and resistance, which are the inheritance of all of us whose bodies and minds will not conform.
01:13:55
Speaker
Those are the 10 principles of disability justice.
01:13:58
Speaker
There's more context inside of this primer.
01:14:00
Speaker
I tried to pull the most salient parts.
01:14:03
Speaker
But wanted to highlight that as the most recent evolution of the work that was cited earlier on in the episode.
01:14:12
Speaker
I guess I'll pass it to you to highlight an org that embodies these principles.
Project LETS: Peer Support and Advocacy
01:14:17
Speaker
Yeah, so Project Let's is essentially peer support for liberated healing.
01:14:24
Speaker
They create peer support collectives, lead political education, and develop new knowledge and language around mental distress and organize and advocate for the liberation process.
01:14:35
Speaker
of community members globally and create innovative peer-led alternatives to our current mental health systems.
01:14:40
Speaker
We talked about the psychiatric survivors movement earlier, and this is an organization that exists right now that, you know, its values are rooted in disability justice as it relates to folks with mental health issues.
01:14:52
Speaker
They fight for self-determination, opportunity,
01:14:56
Speaker
and equity for all disabled, mad, neurodivergent, and mentally ill folks.
01:15:00
Speaker
They do this through offering peer support one-on-one.
01:15:04
Speaker
They also offer community education and speaking.
01:15:08
Speaker
They recently had a workshop for just like individuals of the general public, but also for mental health professionals on a different way of viewing psychosis.
01:15:19
Speaker
They have high school and college chapters to push forward their mission as well and create community education.
01:15:25
Speaker
They have a provider collective that brings together culturally and socially responsive mental health providers to develop a community-based crisis response network that functions as an alternative to calling 911.
01:15:37
Speaker
They have a really beautiful self-harm initiative where they ask people to mail them their tools of self-harm, their razors, their safety pins, their scissors, and
01:15:47
Speaker
and write a letter about their relationship to self-harm and then they will respond with a letter back talking to them about how proud they are of, I guess, sending away their tools.
01:15:58
Speaker
And in April 2023, Project Let's launched their first psychiatric survivor clinic open to anyone who has been harmed by psychiatry.
01:16:06
Speaker
and psychiatric treatment.
01:16:08
Speaker
This space will offer opportunities for community care, peer support, strategizing, and discussion, skill sharing, and co-reflecting.
01:16:15
Speaker
If you want to know more about Project Lutz and support them or attend any of their, you know, events or workshops, you can go to projectlutz.org or find them on Instagram at Project Lutz.
01:16:28
Speaker
This episode was probably cut into two parts.
01:16:33
Speaker
Most definitely cut into two parts.
01:16:34
Speaker
Yes, we've been recording for almost four hours now.
01:16:38
Speaker
So my guess is that both the parts will be about an hour and a half to two hours long.
01:16:43
Speaker
But I hope that you learned a lot about the history of mental health.
01:16:49
Speaker
Started with the West End State Hospital, but branched out into a lot of
01:16:54
Speaker
related tangents that really give us context to where our current mental health systems originate from and why you know so many problems still exist today within our current systems yes
01:17:08
Speaker
As always, take care of yourselves.
01:17:11
Speaker
And if you want to learn more, you can check out the show notes for the references and resources.
01:17:17
Speaker
We shall see you all in the next one.
01:17:19
Speaker
Or you shall hear us in the next one.
01:17:25
Speaker
Catch you next time.
01:17:47
Speaker
Thanks for listening and for supporting us.
01:17:50
Speaker
You can find us on Instagram and Facebook at Unpacking the Eerie, on Twitter at Unpack the Eerie, and on our website at www.unpackingtheerie.com.
01:18:03
Speaker
Yes, and special thanks to all of you who subscribe to our Patreon.
01:18:08
Speaker
As we've mentioned before, we do all the research for this, we edit, and we don't have any sponsorships or ads.
01:18:17
Speaker
So Patreon support is super helpful in just keeping this project sustainable, keeping the Buzzsprout subscription going, paying for the website, all the stuff.
01:18:27
Speaker
So thank you so much.
01:18:29
Speaker
Sari, Liz, Clifton.
01:18:31
Speaker
Jill, Victoria, and Lindsay.
01:18:33
Speaker
Lauren, Vivian, Valerie.
01:18:36
Speaker
Micheline, Montana, Katrina.
01:18:38
Speaker
Raina, Allie, Jake.
01:18:40
Speaker
Drithi, Daphne, and Katie.
01:18:42
Speaker
Vern, Meredith, H, and Vince.
01:18:45
Speaker
To April, Aaron, and Ellen.
01:18:47
Speaker
And to Brittany, Alyssa, and Meredith R. Yay, thank you so much.